
Tuesday, November 1, 2011
Thursday, September 23, 2010

Sunday, May 2, 2010
Journal of Clinical Oncology Reading Notes

The decision to use chemotherapy in addition to hormonal therapy in the treatment of axillary node-negative and estrogen receptor (ER) positive breast cancer should be based not only on baseline risk, but also on prediction of degree of benefit from chemotherapy.
A number of biologic and clinical clues have suggested that not all patients derive the same degree of benefit from chemotherapy. An overview of randomized trials suggests that younger women may benefit more from chemotherapy.
A 21-gene assay has been developed that includes genes involved in tumor cell proliferation and hormonal response, characteristics that have been reported to be associated with chemotherapy response in general.
The recurrence score is calculated on a scale from 0-100 and is derived from the reference-normalized expression measurements for the 16 cancer-related genes (Ki67, STK15, Survivin or BIRC5, CCNB1 of cyclin B1, MYBL2, GRB7, HER2, ER, PGR, BCL2, SCUBE2, MMP11 or stromelysin, CTSL or cathepsin L2, GSTM1, CD68, and BAG1, and the five reference genes.
Patients with node-negative , ER-positive breast cancer in the NSABP B20 study did not benefit equally from chemotherapy. Patients with tumors who had high RS (greater than 31) experienced a large chemotherapy benefit. Patients with tumors that had low RSs derived minimal, if any, benefit from chemotherapy treatment.
For many women with high RSs, the anticipated benefit of adding chemotherapy appears to be very favorable when compared with the risks.
Oncotype DX: Reading Notes

Oncotype DX is a diagnostic test that helps identify which women with early-stage, lymph node negative and estrogen receptor-positive breast cancer are more likely to benefit from adding chemotherapy to their hormonal treatment.
The Oncotype DX test measures the activity of different genes in a woman's breast tissue tumor tissue.
The Oncotype DX test measures the activity of different genes in a woman's breast tissue tumor tissue.
Women with lower (RS) recurrence scores have a lower risk that their cancer will return. These women also have a cancer that is less likely to benefit from chemotherapy. A lower recurrence score does not necessarily mean that there is no chance that the breast cancer will return.
Women with a higher (RS) recurrence score have a stronger chance that their breast cancer will return, but may also benefit largely from chemotherapy. A higher recurrence score does not mean that a woman's breast cancer will definitely return.
Tuesday, April 13, 2010
Identifying perforators in Breast Reconstruction with 3D CT-Scans
The CT-angiogram has shown great utility for DIEP flap, SIEA flap, free TRAM flap, as well as the pedicle TRAM flap in identifying blood supply to the abdominal tissue used in breast reconstruction.

In certain breast reconstruction candidates who have had prior abdominal surgery the CT-angiogram of the abdomen is useful to me not only to plan out the orientation of the flap used in breast reconstruction but also to position the scar on the abdominal wall to facilitate healing.
The illustration below gives an example of a rectus flap planning CT-scan used in breast reconstruction.
Brian P. Dickinson, M.D.
www.drbriandickinson.com
3D CT-Angiogram for Flap Planning in Breast Reconstruction
I have found the CT-angiogram to be very helpful for flap planning in breast reconstruction. The CT-angiogram allows the operative surgeon to have a road map for vessel selection, may facilitate orientation of the flap for breast reconstruction, as well as facilitate positioning of the scar on the abdominal wall for flap harvest.
The CT-angiogram is specifically helpful in the patient who has had previous abdominal operations to determine the integrity of vessels as well as determine which flap may be an appropriate option for the patient such as TRAM, TRAM flap with pre-delay procedure, free TRAM, DIEP, or SIEA.
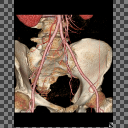
The 3D reconstruction shown below gives an example of how the surgeon can appropriately evaluate vessel integrity in a previously operated abdomen.
Brian P. Dickinson, M.D.
Sunday, January 31, 2010
Deep Inferior Epigastric Perforator Flap Publications

Reconstruction of Total Laryngopharyngectomy Defects with Deep Inferior Epigastric Perforator Flaps:
Otway Louie, Brian Dickinson, Jay Granzow, J. Brian Boyd
Journal of Reconstructive Microsurgery. 25(9):555-558, November 2009
It is truly a great honor and distinct pleasure to publish in the Journal of Reconstructive Microsurgery. I received outstanding microsurgical training from them during my time training at Harbor-UCLA. Deep Inferior Epigastric Artery Perforator Flaps provide well vascularized tissue for distant tissue transfer while minimizing the abdominal donor site.
Subscribe to:
Posts (Atom)